This week, while Congress was on recess, the Trump Administration continued its unprecedented assault on the American health care system. Here’s what happened this week in the Republicans’ war on health care – and the extensive data showing that opposition to the GOP health care agenda is only growing:
SHORT-TERM PLANS? MORE LIKE LONG-TERM SCAMS
On Tuesday, the Trump Administration announced a proposal to let insurance companies sell short-term plans year-round. These plans skirt Affordable Care Act requirements to cover essential health benefits like cancer treatment, substance use treatment, and maternity care and can deny coverage altogether for those with pre-existing conditions.
What do these plans do?
- Short-term health plans offer inadequate medical coverage and circumvent fundamental consumer protections
- Short-term plans provide junk coverage which leaves those who get sick with thousands of dollars in unpaid bills
- Short-term plans offer subpar coverage coverage which will raise premiums and destabilize markets
The negative reactions to this backdoor sabotage came fast and thick:
American Cancer Society Cancer Action Network, American Heart Association, American Liver Foundation, American Lung Association, Arthritis Foundation, Consumers Union, Crohn’s & Colitis Foundation, Cystic Fibrosis Foundation, Epilepsy Foundation, Leukemia And Lymphoma Society, Lutheran Services In America, March Of Dimes, National Health Council, National Ms Society, National Organization For Rare Disorders, United Way, World Wide Volunteers Of America: “The proposed rule released today would permit insurance companies to offer substandard insurance policies to millions of americans… as organizations committed to ensuring that coverage remains affordable, accessible, and adequate for all americans, we cannot support this proposal.” [Consumers Union, 2/20/18]
America’s Health Insurance Plans: “We remain concerned the expanded use of short-term plans could further fragment the individual market, which would lead to higher premiums for many consumers, particularly those with pre-existing conditions.” [Twitter, 2/20/18]
Mike Kreidler, Washington State Insurance Commissioner: “If you get sick you may not be able to renew your coverage — there are no protections for people with pre-existing conditions. maternity care and mental-health benefits often are excluded.” [New York Times, 2/20/18]
Larry Levitt, Kaiser Family Foundation Senior Vice President: “Short-term insurance plans don’t cover pre-existing conditions, don’t cover the aca’s essential benefits, and can impose annual limits on coverage.” [Twitter, 2/20/18]
Rachel Sachs, Health Law Professor: “The government will spend millions more to provide fewer people with comprehensive coverage.” [Twitter, 2/20/18]
REPUBLICANS GO AFTER PRE-EXISTING CONDITIONS
The most popular provision of the Affordable Care Act is its ban on insurance company discrimination against people with pre-existing conditions. Short-term plans would once again force consumers to fill out medical history forms, and pay the price if they check the wrong boxes. Don’t believe us? Take a look at the headlines yourself:
NBC News: Trump pushes insurance that doesn’t cover pre-existing conditions
Vox: Trump’s quiet campaign to bring back preexisting conditions
Alaska Native News: Trump’s Latest Sabotage Targets Americans with Pre-existing Conditions
USA Today: Trump proposes 12-month insurance plans that don’t cover people, issues Obamacare requires
NPR: Trump Administration Wants To Let Insurers Offer Plans With Fewer Benefits
New York Times Editorial Board: Trump Tries to Kill Obamacare by a Thousand Cuts
CAUGHT IN A LIE
Also this week, top Administration health officials Secretary Alex Azar and Administrator Seema Verma directly contradicted their own short-term plan regulation as they desperately tried to spin away the damage which would be inflicted on Americans’ ability to access quality, affordable health care:
| What They Said | What Their Reg Said | |
| Individual market premiums | VERMA: “This shift will have will have virtually no impact on the individual market premiums.” | HHS REG: “It would result in an increase in premiums for the individuals remaining in those risk pools. An increase in premiums for individual market single risk pool coverage would result in an increase in Federal outlays for APTC.” |
| Lower-quality coverage | VERMA: “While in the past these plans have been a bridge, now they can be a lifeline.” | HHS REG: “Consumers who purchase short-term, limited-duration insurance policies and then develop chronic conditions could face financial hardship as a result, until they are able to enroll in PPACA-compliant plans that would provide for such conditions.” |
| Fewer insurance options | AZAR: “This is a group of people, they live in areas of the country where there’s one plan they might have access to, so they’re looking for other options.” | HHS REG: “Individual market issuers could experience higher than expected costs of care and suffer financial losses, which might prompt them to leave the individual market.” |
| Short-term or not? | AZAR: “We are proposing that these plans would be available up to 12 months for people … We are asking for comment on whether we have the legal authority to let people renew their plans.” | HHS REG: “Short-term, limited-duration insurance is a type of health insurance coverage that was designed to fill temporary gaps in coverage that may occur when an individual is transitioning from one plan or coverage to another.” |
| Pre-existing conditions | AZAR: “These plans may have fewer benefits than we’re used to, they may have more restrictions, and also they may be able to limit who they insure for. That’s part of this.” | HHS REG: “Short-term, limited-duration insurance policies would be unlikely to include all the elements of PPACA-compliant plans, such as the preexisting condition exclusion prohibition.” |
CROCODILE TEARS FROM THE SWAMPIEST ADMINISTRATION
On Thursday, Axios reported that America’s largest pharmaceutical companies are using their windfall from the GOP tax scam to drive up their own stock prices to the tune of $50 billion, “a sum that towers over investments in employees or drug research and development.” Why is this so appalling?
- The GOP cried crocodile tears over the cost of prescription drugs – and then gave Big Pharma a giant windfall through their tax scam.
- The GOP has consistently voted to raise prescription drug costs, from the health care repeal that would get rid of Medicare’s prescription drug benefit to their confirmation of a Big Pharma executive who let drug prices skyrocket to lead HHS.
- All the while, millions of Americans continue struggling to afford their prescription drugs, too often being forced to choose between their medication and a meal. And the GOP does nothing.
On prescription drugs, as well as their broader war on health care, however, the GOP’s actions, are finally catching up to them…
AMERICANS AGREE: KEEP YOUR HANDS OFF OUR HEALTH CARE
Four polls over six weeks have reached the same conclusion: the ACA has achieved lasting popularity, the electorate is angry about GOP sabotage, and health care is voters’ top priority. Here’s what the numbers say:
Last week, Public Policy Polling released its first national poll of the year, contrasting the rising popularity of the Affordable Care Act with the blame being leveled on President Trump’s sabotage:
- Approval for the Affordable Care Act is 12 points above water (47% approval to 35% disapproval), a dramatic reversal from trends before Trump took office.
- Over half of voters know Republicans are sabotaging health care, with 51% believing the Trump Administration is actively taking steps that will raise people’s health care costs.
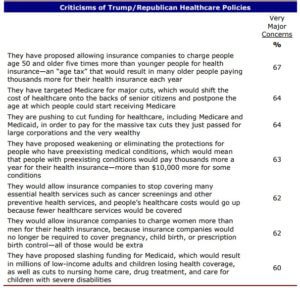
Also last week, a Priorities USA memo found that President Trump’s handling of health care remains vastly unpopular, especially among independent voters:
- On the policy of health care, Donald Trump has a 34/46 favorable/unfavorable message.
- On his handling of drug pricing, 60% of voters have major concerns, including 71% among independents.
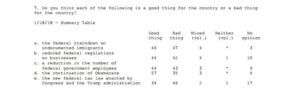
These polls came on the heels of a January Washington Post/ABC News poll asking Americans about President Trump’s time in office, which found that Americans are most united in opposition to the GOP’s health care agenda:
- Asked if keeping “Obamacare” was a good thing for the country, 57 percent of respondents said yes – a significantly higher percentage than any other policy. The only policy underwater? The GOP tax scam, which kicked millions off of their insurance and was opposed 46% – 34%.
And all of these polls followed a Hart Research memo which found health care is the number one issue among voters, far exceeding anything else:
- “Healthcare far exceeds any other issue as an important driver of voting preferences, with over half of all voters identifying healthcare as one of their top priorities in the 2018 congressional elections, with 54% of those surveyed choose health care as one of the two issues that will be the most important to them in deciding how to vote for Congress.”
- Healthcare is the most frequently cited priority among Democrats (68%), independents (54%), and Republicans (38%). It is particularly important to African-American voters (66%) and to white women voters, whether they are college graduates (62%) or non-college graduates (59%).
One poll can be an outlier, two a coincidence – but four polls in six weeks independently highlighting the importance of health care and the contrast between the Affordable Care Act’s popularity and the GOP’s sabotage show just how important this issue is to the American people.
From coast to coast, constituents are making their view abundantly clear: it’s time for the GOP to stop its war on health care, and there will be significant consequences should President Trump and Congressional Republicans fail to heed this advice.