HEADLINES: GOP Bill Guts The Affordable Care Act News HEADLINES: GOP Bill Guts The Affordable Care Act Republicans Are Targeting the ACA in Their Quest to Hand Out Tax Breaks to Billionaires…ashoupJune 3, 2025
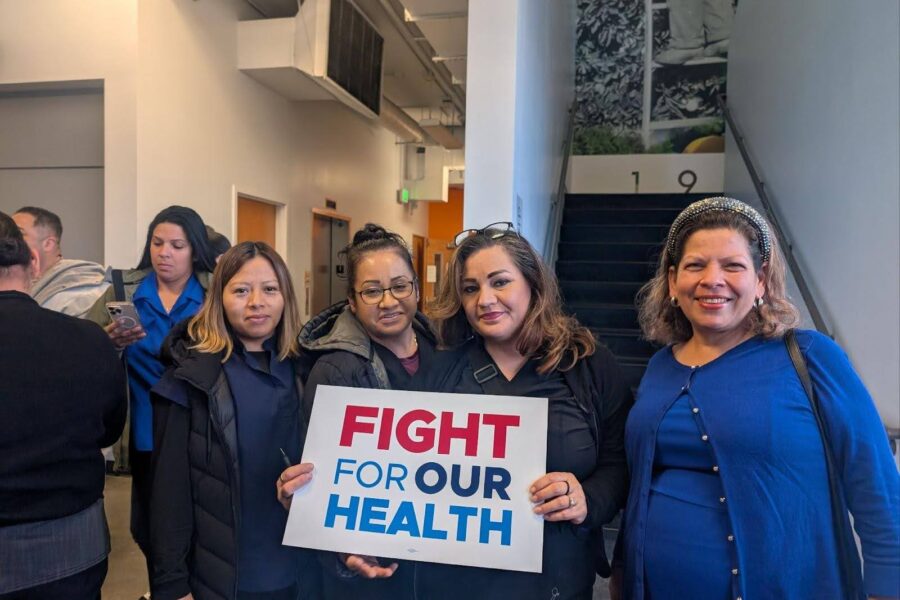
“Wealth Over Workers”: Senator Ron Wyden, Former Medicaid Director Join Protect Our Care to Urge The Senate to Reject the GOP Tax Scam and Protect Health Care for the American People News “Wealth Over Workers”: Senator Ron Wyden, Former Medicaid Director Join Protect Our Care to Urge The Senate to Reject the GOP Tax Scam and Protect Health Care for the American People Watch the Full Event Here. Washington, D.C. — Today, U.S. Senate Finance Committee Ranking Member…ashoupJune 2, 2025
Trump’s War on Health Care: Public Health Watch News Trump’s War on Health Care: Public Health Watch Welcome to Public Health Watch, a weekly roundup from Protect Our Care tracking catastrophic activity…ashoupJune 2, 2025
HEADLINES: Ernst Lets Slip GOP’s Medicaid Agenda – “We’re All Going to Die” – And Then Doubles Down in Sarcastic Apology News HEADLINES: Ernst Lets Slip GOP’s Medicaid Agenda – “We’re All Going to Die” – And Then Doubles Down in Sarcastic Apology On Friday, Republican Senator Joni Ernst (R-IA) exposed the cruelty behind Republicans’ agenda to slash…ashoupJune 2, 2025
PRESS CALL: U.S. Senator Ron Wyden to Join Protect Our Care to Urge The Senate to Reject the GOP Tax Scam and Protect Health Care for the American People NewsPress Call PRESS CALL: U.S. Senator Ron Wyden to Join Protect Our Care to Urge The Senate to Reject the GOP Tax Scam and Protect Health Care for the American People ***MEDIA ADVISORY FOR MONDAY JUNE 2ND AT 3 PM ET*** It’s Up to Senate Republicans…ashoupJune 1, 2025
NEW REPORT: Medicaid Coverage Is at Risk for Millions in the Asian American, Native Hawaiian, and Pacific Islander Community NewsReportResearch NEW REPORT: Medicaid Coverage Is at Risk for Millions in the Asian American, Native Hawaiian, and Pacific Islander Community The GOP Scheme Will Raise Costs and Rip Coverage Away from AANPHI Communities Read the…ashoupMay 30, 2025
NEW: Protect Our Care Launches Ads Holding Republicans’ Feet to the Fire After House Passes Devastating Health Care Cuts News NEW: Protect Our Care Launches Ads Holding Republicans’ Feet to the Fire After House Passes Devastating Health Care Cuts Watch The New Ads Here Washington, D.C. – Protect Our Care is launching new ads…ashoupMay 30, 2025
TODAY: Protect Our Care Holds Events With Sen. Baldwin and Rep. Goldman In States to Call On Republicans to Put an End to Their War on American Health Care NewsPress Call TODAY: Protect Our Care Holds Events With Sen. Baldwin and Rep. Goldman In States to Call On Republicans to Put an End to Their War on American Health Care ***MEDIA ADVISORY FOR MAY 29*** Protect Our Care Holds Events In New York, South Dakota,…ashoupMay 29, 2025
HEADLINES: Republicans Face Blowback For Slashing Medicaid After Passing Devastating Budget Bill NewsRoundup HEADLINES: Republicans Face Blowback For Slashing Medicaid After Passing Devastating Budget Bill The Pressure Is On Republican Senators to Reject House Reconciliation Bill and Protect Health Care…ashoupMay 27, 2025
Trump’s War on Health Care: Public Health Watch News Trump’s War on Health Care: Public Health Watch Welcome to Public Health Watch, a weekly roundup from Protect Our Care tracking catastrophic activity…ashoupMay 27, 2025